
Anti-Bacterial Action of Plasma Multi-Jets in the Context of Chronic Wound Healing


 ,
,  , ,
, ,
Abstract
:Featured Application
Abstract
1. Introduction
2. Materials and Methods
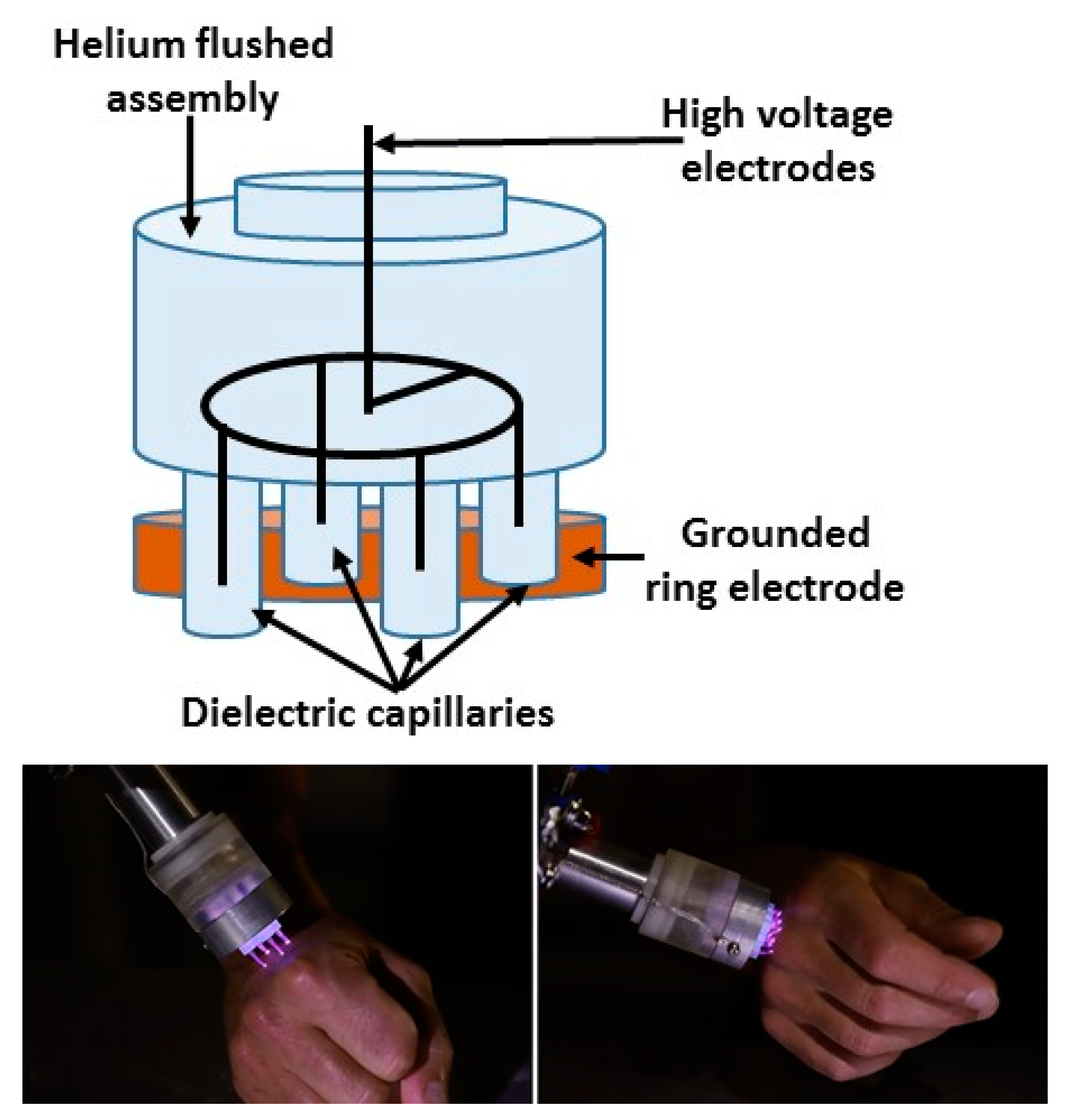
2.1. Plasma Jet Devices
2.2. Biological Samples
2.2.1. Bacterial Lawn Preparation and Plasma Treatment
2.2.2. Bacterial Strains
2.2.3. Agar Samples for Multi-Jets Characterization
2.3. Current Measurement
3. Results
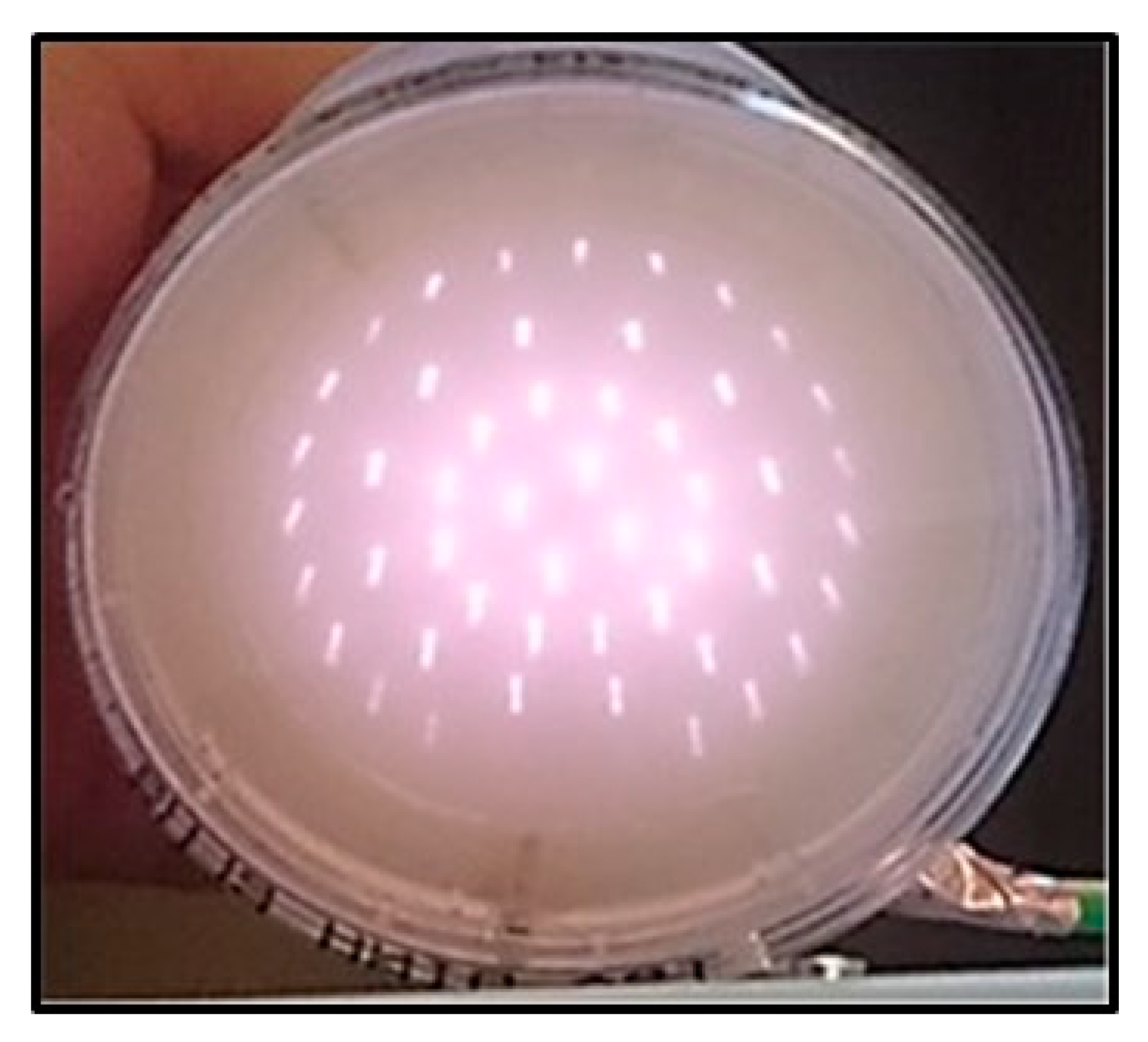
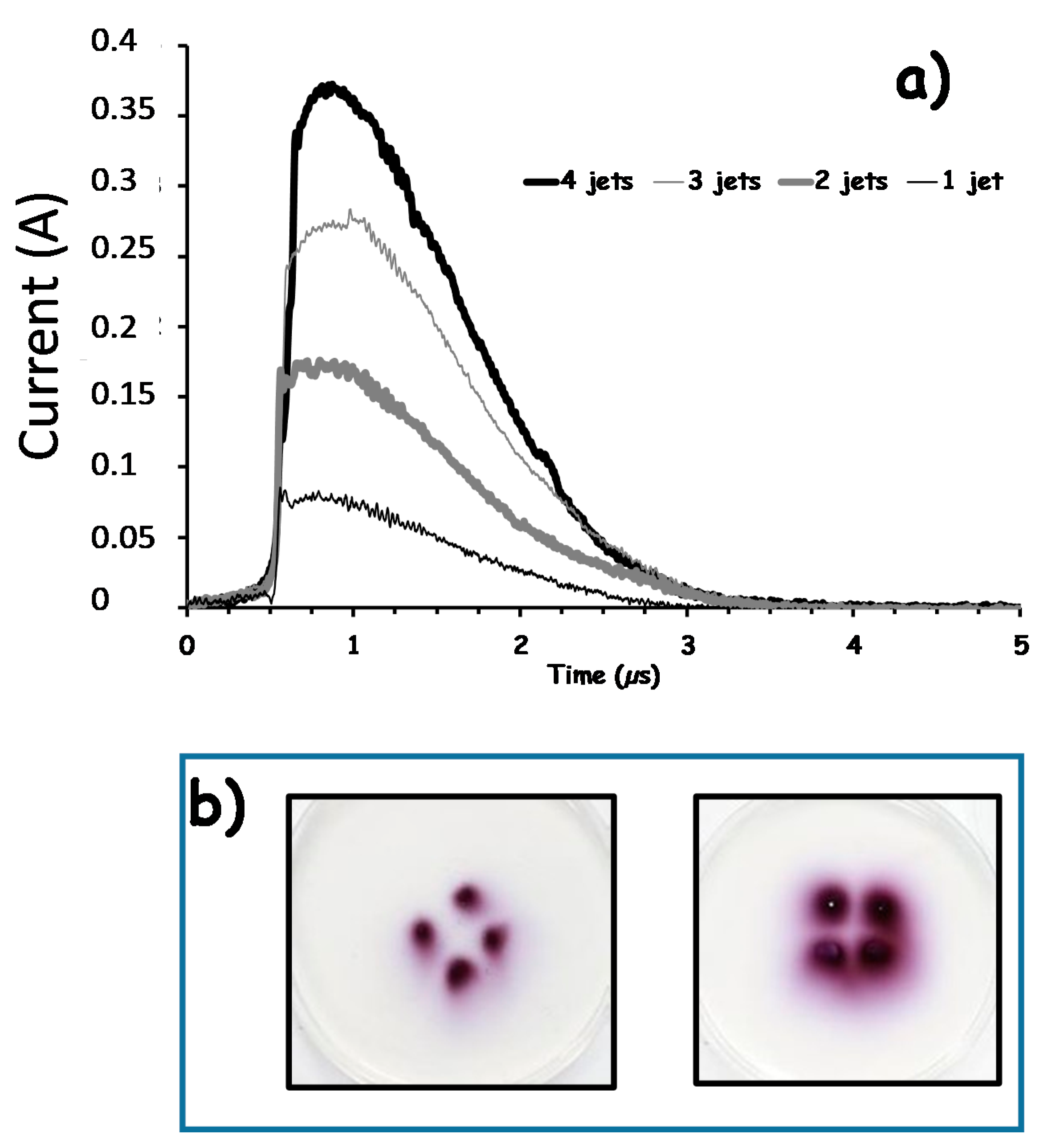
3.1. Multi-Jets Characterization
3.2. Inactivation of Staphylococcus aureus
3.3. Inactivation of Pseudomonas aeruginosa ATCC®9027TM and Resistant Pseudomonas aeruginosa Cultured from Patient’s Sampling
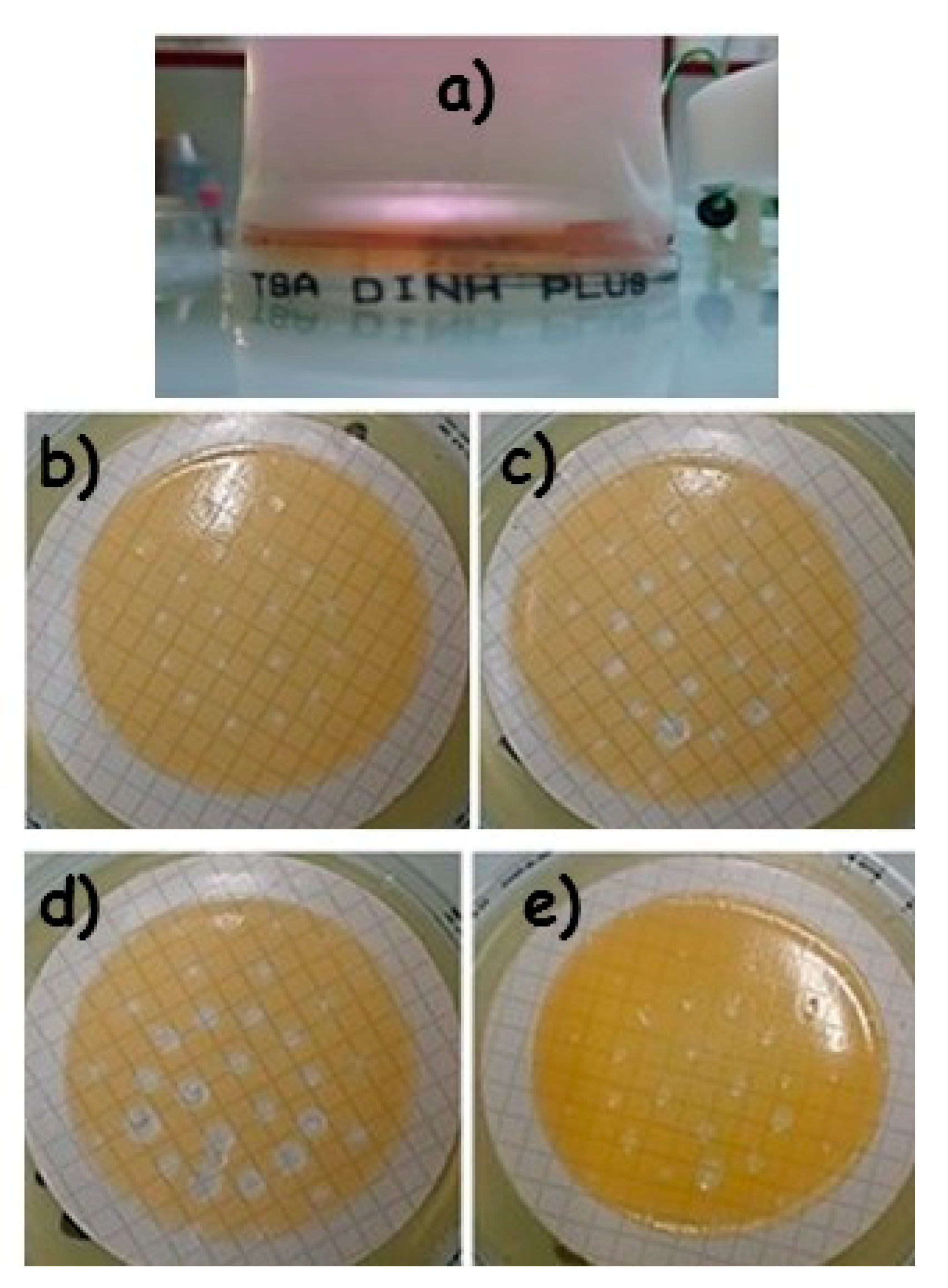
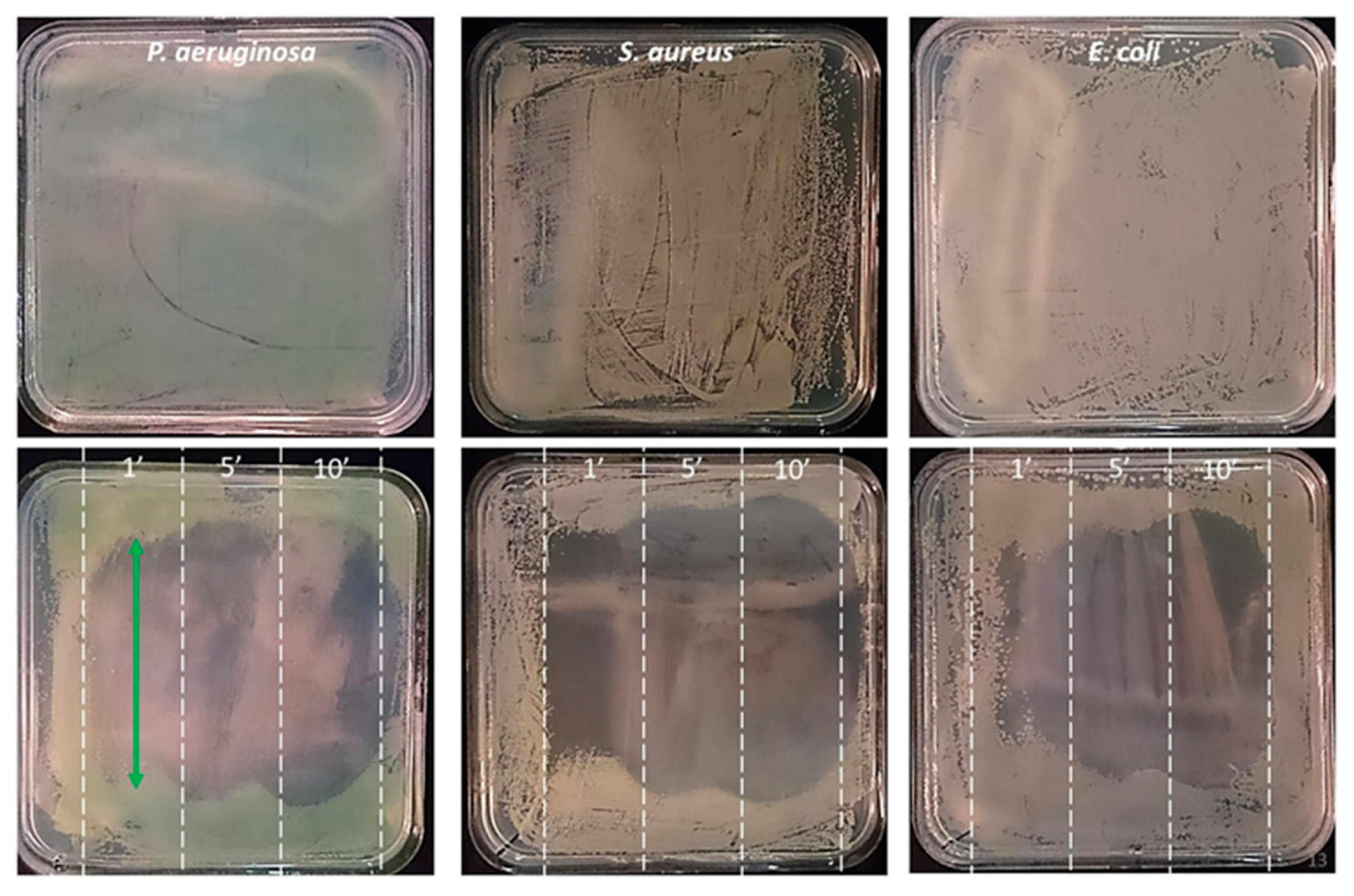
3.4. Large Surface Resistant Bacterial Lawn Inactivation with Scanning Protocols
3.5. Pilot Tolerance Study on the Use of Plasma Therapy for Wound Treatment
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Laroussi, M. Nonthermal decontamination of biological media by atmospheric-pressure plasmas: Review, analysis, and prospects. IEEE Trans. Plasma Sci. 2002, 30, 1409–1415. [Google Scholar] [CrossRef]
- Moisan, M.; Barbeau, J.; Moreau, S.; Pelletier, J.; Tabrizian, M.; Yahia, L. Low-temperature sterilization using gas plasmas: A review of the experiments and an analysis of the inactivation mechanisms. Int. J. Pharm. 2001, 226, 1–21. [Google Scholar] [CrossRef]
- Menaschi, W.P. Treatment of Surfaces. U.S. Patent 3,383,163, 14 May 1968. [Google Scholar]
- Jacobs, P.T.; Lin, S.M. Gas-plasma sterilization. In Irradiation of Polymers: Fundamentals and Technological Applications; Cough, R., Shalaby, S., Eds.; American Chemical Society: Washington, DC, USA, 1994. [Google Scholar]
- Crow, S.; Smith, J.H., III. Gas Plasma Sterilization—Application of Space-Age Technology. Infect. Control. Hosp. Epidemiol. 1995, 16, 483–487. [Google Scholar] [CrossRef] [PubMed]
- Deilmann, M.; Halfmann, H.; Bibinov, N.; Wunderlich, J.; Awakowicz, P. Low-Pressure Microwave Plasma Sterilization of Polyethylene Terephthalate Bottles. J. Food Prot. 2008, 71, 2119–2123. [Google Scholar] [CrossRef] [PubMed]
- Ehlbeck, J.; Schnabel, U.; Polak, M.; Winter, J.; Von Woedtke, T.; Brandenburg, R.; Hagen, T.V.D.; Weltmann, K.-D. Low temperature atmospheric pressure plasma sources for microbial decontamination. J. Phys. D Appl. Phys. 2010, 44. [Google Scholar] [CrossRef] [Green Version]
- Belgacem, Z.B.; Carré, G.; Charpentier, E.; Le-Bras, F.; Maho, T.; Robert, E.; Pouvesle, J.-M.; Polidor, F.; Gangloff, S.C.; Boudifa, M.; et al. Innovative non-thermal plasma disinfection process inside sealed bags: Assessment of bactericidal and sporicidal effectiveness in regard to current sterilization norms. PLoS ONE 2017, 12, e0180183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bekeschus, S.; Favia, P.; Robert, E.; von Woedtke, T. White paper on plasma for medicine and hygiene: Future in plasma health sciences. Plasma Process. Polym. 2019, 16, 1800033. [Google Scholar] [CrossRef] [Green Version]
- Yadav, B.; Spinelli, A.C.; Misra, N.N.; Tsui, Y.Y.; McMullen, L.M.; Roopesh, M.S. Effect of in-package atmospheric cold plasma discharge on microbial safety and quality of ready-to-eat ham in modified atmospheric packaging during storage. J. Food Sci. 2020, 85, 1203–1212. [Google Scholar] [CrossRef]
- Emerald, A.M.; Emerald, L.; Emerald, V.; Kumar, V. Perspective of natural products in skincare. Pharm. Pharmacol. Int. J. 2016, 4, 72. [Google Scholar]
- Capelli, S.F.; Tappi, T.; Gritti, A.C.; de Aguiar Saldanha Pinheiro, R.; Laurita, U.; Tylewicz, F.; Spataro, G.; Braschi, R.; Lanciotti, F.; Gómez Galindo, V.; et al. Decontamination of food packages from SARS-COV-2 RNA with a cold plasma-assisted system. Appl. Sci. 2021, 11, 4177. [Google Scholar] [CrossRef]
- Bekeschus, S.; Kramer, A.; Suffredini, E.; Von Woedtke, T.; Colombo, V. Gas Plasma Technology—An Asset to Healthcare During Viral Pandemics Such as the COVID-19 Crisis? IEEE Trans. Radiat. Plasma Med Sci. 2020, 4, 391–399. [Google Scholar] [CrossRef]
- Fridman, G.G.; Friedman, A.; Gutsol, A.B.; Shekhter, V.N.; Vasilets, A.; Fridman, A. Applied plasma medicine. Plasma Process. Polym. 2008, 5, 503–533. [Google Scholar] [CrossRef]
- Kong, M.; Kroesen, G.; Morfill, G.; Nosenko, T.; Shimizu, T.; Van Dijk, J.; Zimmermann, J.L. Plasma medicine: An introductory review. New J. Phys. 2009, 11, 1–35. [Google Scholar] [CrossRef]
- Isbary, G.; Morfill, G.; Schmidt, H.; Georgi, M.; Ramrath, K.; Heinlin, J.; Karrer, S.; Landthaler, M.; Shimizu, T.; Steffes, B.; et al. A first prospective randomized controlled trial to decrease bacterial load using cold atmospheric argon plasma on chronic wounds in patients. Br. J. Dermatol. 2010, 163, 78–82. [Google Scholar] [CrossRef] [PubMed]
- Nastuta, A.V.; Topala, I.; Grigoras, C.; Pohoata, V.; Popa, G. Stimulation of wound healing by helium atmospheric pressure plasma treatment. J. Phys. D Appl. Phys. 2011, 44, 105204. [Google Scholar] [CrossRef] [Green Version]
- Emmert, F.S.; Brehmer, H.; Hänßle, A.; Helmke, N.; Mertens, R.; Ahmed, D.; Simon, D.; Wandke, W.; Maus-Friedrichs, G.; Däschlein, M.P.; et al. Atmospheric pressure plasma in dermatology: Ulcus treatment and much more. Clin. Plasma Med. 2013, 1, 24–29. [Google Scholar] [CrossRef]
- Alcantara, E.G.; López-Callejas, R.; Morales-Ramírez, P.R.; Peña-Eguiluz, R.; Fajardo, R.; Mercado-Cabrera, A.; Barocio, S.R.; Valencia-Alvarado, R.; Rodriguez-Mendez, B.G.; Muñoz-Castro, A.E.; et al. Accelerated Mice Skin Acute Wound Healing In Vivo by Combined Treatment of Argon and Helium Plasma Needle. Arch. Med. Res. 2013, 44, 169–177. [Google Scholar] [CrossRef] [PubMed]
- BHaertel, B.; Von Woedtke, T.; Weltmann, K.-D.; Lindequist, U. Non-Thermal Atmospheric-Pressure Plasma Possible Application in Wound Healing. Biomol. Ther. 2014, 22, 477–490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmidt, A.; Bekeschus, S.; Wende, K.; Vollmar, B.; von Woedtke, T. A cold plasma jet accelerates wound healing in a murine model of full-thickness skin wounds. Exp. Dermatol. 2017, 26, 156–162. [Google Scholar] [CrossRef]
- Gweon, B.; Kim, K.; Choe, W.; Shin, J.H. Therapeutic uses of atmospheric pressure plasma: Cancer and wound. In Biomedical Engineering: Frontier Research and Converging Technologies; Springer: Berlin/Heidelberg, Germany, 2016; pp. 357–385. [Google Scholar]
- Douat, C.; Bocanegra, P.E.; Dozias, S.; Robert, É.; Motterlini, R. Production of carbon monoxide from a He/CO2 plasma jet as a new strategy for therapeutic applications. Plasma Process. Polym. 2021, 18, e2100069. [Google Scholar] [CrossRef]
- Vandamme, M.; Robert, E.; Pesnel, S.; Barbosa, E.; Dozias, S.; Sobilo, J.; Lerondel, S.; Le Pape, A.; Pouvesle, J.-M. Antitumor Effect of Plasma Treatment on U87 Glioma Xenografts: Preliminary Results. Plasma Process. Polym. 2010, 7, 264–273. [Google Scholar] [CrossRef]
- Keidar, M.; Walk, R.M.; Shashurin, A.; Srinivasan, P.; Sandler, A.; Dasgupta, S.; Ravi, R.; Guerrero-Preston, R.; Trink, B. Cold plasma selectivity and the possibility of a paradigm shift in cancer therapy. Br. J. Cancer 2011, 105, 1295–1301. [Google Scholar] [CrossRef] [PubMed]
- Miller, A.V.; Lin, A.; Fridman, A. Why target immune cells for plasma treatment of cancer? Plasma Chem. Plasma Process. 2016, 36, 259–268. [Google Scholar] [CrossRef]
- Rasouli, M.; Mehdian, H.; Hajisharifi, K.; Amini, E.; Ostrikov, K.; Robert, E. Plasma-activated medium induces apoptosis in chemotherapy-resistant ovarian cancer cells: High selectivity and synergy with carboplatin. Plasma Process. Polym. 2021, 18, e2100074. [Google Scholar] [CrossRef]
- Brullé, M.L.; Vandamme, D.; Riès, E.; Martel, E.; Robert, S.; Lerondel, V.; Trichet, S.; Richard, J.-M.; Pouvesle, A.l. Effects of a non-thermal plasma treatment alone or in combination with gemcitabine in a MIA PaCa2-luc orthotopic pancreatic carcinoma model. PLoS ONE 2012, 7, e52653. [Google Scholar] [CrossRef]
- Schlegel, J.J.; Köritzer, V.; Boxhammer, V. Plasma in cancer treatment. Clin. Plasma Med. 2013, 1, 2–7. [Google Scholar] [CrossRef]
- Bekeschus, S.; Masur, K.; Kolata, J.; Wende, K.; Schmidt, A.; Bundscherer, L.; Barton, A.; Kramer, A.; Bröker, B.; Weltmann, K.-D. Human Mononuclear Cell Survival and Proliferation is Modulated by Cold Atmospheric Plasma Jet. Plasma Process. Polym. 2013, 10, 706–713. [Google Scholar] [CrossRef]
- Szili, E.J.; Oh, J.-S.; Fukuhara, H.; Bhatia, R.; Gaur, N.; Nguyen, C.K.; Hong, S.H.; Ito, S.; Ogawa, K.; Kawada, C.; et al. Modelling the helium plasma jet delivery of reactive species into a 3D cancer tumour. Plasma Sources Sci. Technol. 2017, 27, 014001. [Google Scholar] [CrossRef] [Green Version]
- Brun, P.; Bernabè, G.; Marchiori, C.; Scarpa, M.; Zuin, M.; Cavazzana, R.; Zaniol, B.; Martines, E. Antibacterial efficacy and mechanisms of action of low power atmospheric pressure cold plasma: Membrane permeability, biofilm penetration and antimicrobial sensitization. J. Appl. Microbiol. 2018, 125, 398–408. [Google Scholar] [CrossRef]
- Sakudo, A.; Misawa, T. Antibiotic-Resistant and Non-Resistant Bacteria Display Similar Susceptibility to Dielectric Barrier Discharge Plasma. Int. J. Mol. Sci. 2020, 21, 6326. [Google Scholar] [CrossRef]
- Joshi, S.G.; Paff, M.; Friedman, G.; Fridman, G.; Fridman, A.; Brooks, A.D. Control of methicillin-resistant Staphylococcus aureus in planktonic form and biofilms: A biocidal efficacy study of nonthermal dielectric-barrier discharge plasma. Am. J. Infect. Control. 2010, 38, 293–301. [Google Scholar] [CrossRef] [PubMed]
- Klämpfl, T.G.; Shimizu, T.; Koch, S.; Balden, M.; Gemein, S.; Li, Y.-F.; Mitra, A.; Zimmermann, J.L.; Gebel, J.; Morfill, G.E.; et al. Decontamination of Nosocomial Bacteria IncludingClostridium difficileSpores on Dry Inanimate Surface by Cold Atmospheric Plasma. Plasma Process. Polym. 2014, 11, 974–984. [Google Scholar] [CrossRef]
- He, Y.; Ding, C.; Jin, T.; Fan, Y.; Wu, Z.; Sun, M.; Wang, K.; Ji, T. Sensitivity of two drug-resistant bacteria to low-temperature air plasma in catheter-associated urinary tract infections under different environments. Plasma Sci. Technol. 2020, 22, 065502. [Google Scholar] [CrossRef]
- Stancampiano, A.; Gallingani, T.; Gherardi, M.; Machala, Z.; Maguire, P.; Colombo, V.; Pouvesle, J.-M.; Robert, E. Plasma and Aerosols: Challenges, Opportunities and Perspectives. Appl. Sci. 2019, 9, 3861. [Google Scholar] [CrossRef] [Green Version]
- Bisag, A.; Isabelli, P.; Laurita, R.; Bucci, C.; Capelli, F.; Dirani, G.; Gherardi, M.; Laghi, G.; Paglianti, A.; Sambri, V.; et al. Cold atmospheric plasma inactivation of aerosolized microdroplets containing bacteria and purified SARS-CoV-2 RNA to contrast airborne indoor transmission. Plasma Process. Polym. 2020, 17. [Google Scholar] [CrossRef]
- Chiappim, W.; Sampaio, A.; Miranda, F.; Petraconi, G.; Sobrinho, A.D.S.; Cardoso, P.; Kostov, K.; Koga-Ito, C.; Pessoa, R. Nebulized plasma-activated water has an effective antimicrobial effect on medically relevant microbial species and maintains its physicochemical properties in tube lengths from 0.1 up to 1.0 m. Plasma Process. Polym. 2021, e2100010. [Google Scholar] [CrossRef]
- Daeschlein, G.; Napp, M.; Lutze, S.; Arnold, A.; Von Podewils, S.; Guembel, D.; Jünger, M. Skin and wound decontamination of multidrug-resistant bacteria by cold atmospheric plasma coagulation. J. der Dtsch. Dermatol. Ges. 2015, 13, 143–149. [Google Scholar] [CrossRef]
- Heinlin, J.; Isbary, G.; Stolz, W.; Morfill, G.; Landthaler, M.; Shimizu, T.; Steffes, B.; Nosenko, T.; Zimmermann, J.; Karrer, S. Plasma applications in medicine with a special focus on dermatology. J. Eur. Acad. Dermatol. Venereol. 2010, 25, 1–11. [Google Scholar] [CrossRef]
- Pouvesle, C.J.-M.; Cachoncinlle, R.; Viladrosa, A.; Khacef, E.; Robert, S.; Dozias, S. Transient Plasma Ball Generation System at Long Distance. U.S. Patent 8,482,206, 9 July 2013. [Google Scholar]
- Pouvesle, E.J.-M.; Robert, S.; Dozias, M.; Hugnot, V.; Sarron, T.; Darny, T. Method and Device for Generating a Plurality of Cold-Plasma Jets at Atmospheric Pressure. U.S. Patent 10,420,852, 24 September 2019. [Google Scholar]
- Omran, A.V.; Busco, G.; Ridou, L.; Dozias, S.; Grillon, C.; Pouvesle, J.-M.; Robert, E. Cold atmospheric single plasma jet for RONS delivery on large biological surfaces. Plasma Sources Sci. Technol. 2020, 29, 105002. [Google Scholar] [CrossRef]
- Robert, E.; Darny, T.; Dozias, S.; Iséni, S.; Pouvesle, J.M. New insights on the propagation of pulsed atmospheric plasma streams: From single jet to multi jet arrays. Phys. Plasmas 2015, 22, 122007. [Google Scholar] [CrossRef] [Green Version]
- Lietz, A.M.; Damany, X.; Robert, E.; Pouvesle, J.-M.; Kushner, M.J. Ionization wave propagation in an atmospheric pressure plasma multi-jet. Plasma Sources Sci. Technol. 2019, 28, 125009. [Google Scholar] [CrossRef]
- Kostov, K.; Machida, M.; Prysiazhnyi, V.; Honda, R.Y. Transfer of a cold atmospheric pressure plasma jet through a long flexible plastic tube. Plasma Sources Sci. Technol. 2015, 24. [Google Scholar] [CrossRef]
- Chung, A.T.H.; Stancampiano, K.; Sklias, K.; Gazeli, F.M.; André, S.; Dozias, C.; Douat, J.-M.; Pouvesle, J.; Santos Sousa, E.; Robert, L.M. Mir, Cell electropermeabilisation enhancement by non-thermal-plasma-treated pbs. Cancers 2020, 12, 219. [Google Scholar] [CrossRef] [Green Version]
- Szili, J.S.E.J.; Oh, S.H.; Hong, A.; Hatta, R.D. Short, Probing the transport of plasma generated RONS in an agarose target as surrogate for real tissue: Dependency on time, distance and material composition. J. Phys. D Appl. Phys. 2015, 48, 202001. [Google Scholar] [CrossRef]
- Kawasaki, F.T.; Mitsugi, F.; Koga, M.K.; Shiratani, M. Local supply of reactive oxygen species into a tissue model by atmospheric-pressure plasma-jet exposure. J. Appl. Phys. 2019, 125, 213303. [Google Scholar] [CrossRef]
- Vandamme, M.; Robert, E.; Lerondel, S.; Sarron, V.; Ries, D.; Dozias, S.; Sobilo, J.; Gosset, D.; Kieda, C.; Legrain, B.; et al. ROS implication in a new antitumor strategy based on non-thermal plasma. Int. J. Cancer 2012, 130, 2185–2194. [Google Scholar] [CrossRef]
- Graves, D.B. The emerging role of reactive oxygen and nitrogen species in redox biology and some implications for plasma applications to medicine and biology. J. Phys. D Appl. Phys. 2012, 45. [Google Scholar] [CrossRef]
- Sobota, A.; Guaitella, O.; Garcia-Caurel, E. Experimentally obtained values of electric field of an atmospheric pressure plasma jet impinging on a dielectric surface. J. Phys. D Appl. Phys. 2013, 46. [Google Scholar] [CrossRef]
- Orr, K.; Tang, Y.; Simeni, M.S.; Bekerom, D.V.D.; Adamovich, I.V. Measurements of electric field in an atmospheric pressure helium plasma jet by the E-FISH method. Plasma Sources Sci. Technol. 2020, 29, 035019. [Google Scholar] [CrossRef]
- Bourdon, T.A.; Darny, F.; Pechereau, J.-M.; Pouvesle, P.; Viegas, S.; Iséni, E.; Robert, E. Numerical and experimental study of the dynamics of a μs helium plasma gun discharge with various amounts of N2 admixture. Plasma Sources Sci. Technol. 2016, 25, 035002. [Google Scholar] [CrossRef]
- Xiong, Z.; Kushner, M.J. Atmospheric pressure ionization waves propagating through a flexible high aspect ratio capillary channel and impinging upon a target. Plasma Sources Sci. Technol. 2012, 21. [Google Scholar] [CrossRef]
- Dozias, J.-M.S.; Pouvesle, E.; Robert, E. Comment on ‘Mapping the electric field vector of guided ionization waves at atmospheric pressure’ 2020 Plasma Res. Express 2 025014. Plasma Res. Express 2021, 3, 038001. [Google Scholar] [CrossRef]
- Vijayarangan, V.; Delalande, A.; Dozias, S.; Pouvesle, J.-M.; Robert, E.; Pichon, C. New insights on molecular internalization and drug delivery following plasma jet exposures. Int. J. Pharm. 2020, 589, 119874. [Google Scholar] [CrossRef]
- Van der Paal, J.; Fridman, G.; Bogaerts, A. Ceramide cross-linking leads to pore formation: Potential mechanism behind CAP enhancement of transdermal drug delivery. Plasma Process. Polym. 2019, 16, 1900122. [Google Scholar] [CrossRef]
- Jinno, M.; Ikeda, Y.; Motomura, H.; Kido, Y.; Satoh, S. Investigation of plasma induced electrical and chemical factors and their contribution processes to plasma gene transfection. Arch. Biochem. Biophys. 2016, 605, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Zhuang, J.; von Woedtke, T.; Kolb, J.F.; Zhang, J.; Fang, J.; Weltmann, K.-D. Synergistic antibacterial effects of treatments with low temperature plasma jet and pulsed electric fields. Appl. Phys. Lett. 2014, 105, 104103. [Google Scholar] [CrossRef]
- Mir, L.M. Recommendations for plasma multi-jets usage: Summary of pilot mouse stud. In French, Private Communication; Internal Report PEPS ACUMULTIPLAS’s Project; France, 2018. [Google Scholar]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1st Option Single Jet | 2nd Option Multi-Jets From One Primary Jet | 3rd Option Bunch of Individual Jets | ||
|---|---|---|---|---|
| Voltage (kV) | 10–20 | 14 | 3 | |
| Repetition rate (kHz) | 20 | 2 | 10–20 | |
| Gas flow (L/min) | 0.5 | 4 | 3 | |
| Key advantage | Simplest design | Large surface treatment | Less sensitive to target distance topology | |
| Name of the plasma applicator | Single jet | Multi spot | Diffuse mode | Low voltage |
| Plasma impact | One two mm spot moving over a 2 cm2 disk | 4 + 12 + 12 + 24, one mm spots distributed over 8/18/28/38 mm in diameter rings | Same as multi spot with additional diffuse volume between the multi jets | 4/9/13 two mm spots distributed over a 2/3/3 in diameter disk |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maho, T.; Binois, R.; Brulé-Morabito, F.; Demasure, M.; Douat, C.; Dozias, S.; Escot Bocanegra, P.; Goard, I.; Hocqueloux, L.; Le Helloco, C.; et al. Anti-Bacterial Action of Plasma Multi-Jets in the Context of Chronic Wound Healing. Appl. Sci. 2021, 11, 9598. https://doi.org/10.3390/app11209598
Maho T, Binois R, Brulé-Morabito F, Demasure M, Douat C, Dozias S, Escot Bocanegra P, Goard I, Hocqueloux L, Le Helloco C, et al. Anti-Bacterial Action of Plasma Multi-Jets in the Context of Chronic Wound Healing. Applied Sciences. 2021; 11(20):9598. https://doi.org/10.3390/app11209598
Chicago/Turabian StyleMaho, Thomas, Raphaelle Binois, Fabienne Brulé-Morabito, Maryvonne Demasure, Claire Douat, Sébastien Dozias, Pablo Escot Bocanegra, Isabelle Goard, Laurent Hocqueloux, Claire Le Helloco, and et al. 2021. "Anti-Bacterial Action of Plasma Multi-Jets in the Context of Chronic Wound Healing" Applied Sciences 11, no. 20: 9598. https://doi.org/10.3390/app11209598